
![]()
Spontaneous cardiomyopathy resembling acute rheumatic heart disease in anowl monkey
![]()
Gozalo A, Dagle GE, Montoya E, Weller RE. Spontaneous cardiomyopa thy resembling acute rheumatic heart disease in an owl monkey. J Med Priniatol 1992:21:381-383. A wild-caught male Aotus vociferans died spontaneously during quarantine. Histologic examination of the heart showed several small myocardial arteries replaced with fibrinoid necrosis and adjacent inflammation that included lymphocytes and large histiocytic cells. Less often, similar inflammatory foci were observed in the myocardium interstitium. The lesions observed in the heart of the owl monkey resembled Aschoff bodies.
Alfonso Gozalo1, Gerald E.
Dagle2 Enrique Montoya, 1
Richard E. Weller 2
1Center for Reproduction and Conservation of Non Human Primates,
Instituto Veterinario de Investigaciones Tropicales y de Altura, Universidad
Nacional Mayor de San Marcos, Iquitos, Perú; 2Battelle
Corporation, Pacific Northwest Laboratories, Richland, WA, U.S.A.
Key words: primate-cebidae-Aotus vociferans-cardiomyopathy-fibrinoid necrosis
Alfonso Gozalo, DVM, Unidad de Post Grado, Facultad de Medicina Veterinaria, Univ. Nac. Mayor de San Marcos, Apartado 03-5137, Correo de Salamanca, Lima, Peru.
Accepted for publication June 3, 1992.
Introduction
![]()
In this report we describe a case of spontaneous cardiomyopathy resembling acute rheumatic heart
disease in an owl monkey.
Case report
A subadult male owl monkey (Aotus vociferans) (No. 2211), weighing 750g, arrived at the Center for Reproduction and Conservation of Non Human Primates (CRCP) in Iquitos, Peru, on August 14, 1989, along with 16 wild-caught A. vociferans from the Peruvian Amazonia. The monkey was wildcaught one week earlier in the Nanay river basin. The monkeys were TB tested during quarantine and were all negative. After 38 days in quarantine, the Aotus 2211 died unexpectedly.
At postmortem examination, the monkey weighed 840g, and was in good general condition. The lungs, liver, kidneys, and gastrointestinal mucosa were congested. The spleen was slightly pate. All other organs appeared normal. Tissue samples of all major organs were taken and fixed in 10% neutral buffered formalin and processed routinely for hematoxylin and eosin staining. Tissue samples from lungs, liver, and intestine were taken for microbiological analysis following established techniques [2].
|
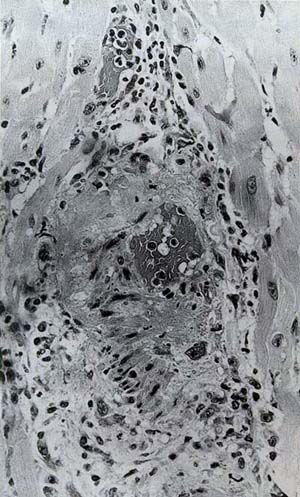
Fig. 1. Small myocardial artery replaced with fibrinous eosinophilic necrosis and associated adjacent inflammation that included some lymphocytes and large histiocytic cells with large nuclei and prominent nucleoli (arrow). H&E, x 250. |
At histopathologic examination, the heart showed several small myocardial arteries replaced with fibrinous eosinophilic necrosis and some associated adjacent inflammation that included some lymphocytes and large histiocytic cells with large nuclei and centrally disposed prominent chromatin (Fig. 1). The eosinophilic material resembled fibrinoid necrosis. Less often, similar lesions were observed in the myocardium interstitium. One histiocyte with large nuclei and ribbon-like disposition of chromatin resembling an Anitschkow cell was observed in a lesion (Fig. 2). These focal areas of inflammation in the myocardium resembled Aschoff bodies. Additionally, fibrinoid necrosis of small follicular arteries were found in the spleen. The small intestinal mucosa presented moderate diffuse increased mixed cellular infiltration in the glands that included plasma cells and eosinophils. There were also mixed inflammatory cells in the submucosa with associated congestion and some fibrinoid necrosis in the walls of small arteries. All other organs were normal. Bacteriological cultures revealed Escherichia coli, Enterobacter agglomerans, and monilia in the intestine, and E. agglomerans and Gram-negative cocci in lungs. No bacteria were isolated from liver. The microorganisms isocontaminants, and those isolated from intestine are considered normal inhabitants of the intestinal microflora.
 |
Fig. 2. Histiocyte with large nuclei and ribbon-like disposition of chromatin resembling an Anitschkow cell (arrow). H&E,x 625. |
Discussion Group A streptococcal infections have been induced experimentally in the throat and the skin of baboons and chimpanzees, but the relatively severe infections obtained in these animals were not observed to result in development of sequela of streptococcal infection like those observed in man after naturally occurring infections [1]. Although chimpanzees often have high titers of streptococcal antibodies without experimental,inoculation with streptococci, no evidence of rheumatic fever was observed [1]. No other examples of naturally occurring streptococcal infection other than in chimpanzees was found in primatological literature.
Lesions observed in the heart of the owl monkey reported here resembled Aschoff bodies. Additionally, fibrinoid necrosis of small arteries were foundin other organs. No infection with hemolytic streptococci, however, was determined; pharyngeal microbiological analysis was not performed and a possible source of infection was not established. The pharyngeal samples were not taken for microbiological analysis because rheumatic heart disease was not suspected at necropsy. Thus, our suspicion of acute rheumatic heart disease cannot be confirmed by isolation of the etiologic agent, the group A streptococci.
